
PCOS treatment for fertility can feel like a huge, tangled mess. Your hormones do their own thing, your period shows up whenever it wants, or not at all, and everyone online has an opinion about what you should do next. Let’s just pause for a second:
If you’re dealing with PCOS and trying to get pregnant, you’re not broken. You’re not “too hormonal.” Your body just needs the right kind of support, and a plan that actually fits you, not a random list from someone’s Instagram story. This piece on Hormonal Imbalance and Back Pain: The Surprising Connection is a good example of how hormones like to show up in places you wouldn’t expect.
This guide cuts through the noise. We’ll get into the most common questions about PCOS and fertility in plain English. No sugarcoating, no medical jargon. Just real talk about what actually helps.
How to Get Pregnant with PCOS
If you’re searching for how to get pregnant with PCOS, you’re definitely not alone. It’s one of the most common questions people ask after a diagnosis, and for good reason. PCOS can make ovulation less predictable, but it doesn’t mean pregnancy is out of reach
Let’s keep it real: the goal is usually ovulation. Not “perfect hormones.” Not “zero symptoms.” Just getting your body to release an egg more regularly.
So if you’re asking how to get pregnant with polycystic ovaries, start here:
Your doctor will usually look at whether you’re ovulating at all, how often, and what else might be in the way (thyroid stuff, prolactin, sperm factors, blocked tubes, the whole party). Then you build a plan around the actual problem, not generic PCOS advice.
And yes, lifestyle support matters too. Not in a preachy way. In a “let’s stop your blood sugar from acting like a toddler on a sugar high” kind of way.
What is PCOS and how does it mess with fertility?
PCOS (polycystic ovary syndrome) is a hormone imbalance that throws your ovaries off balance.
Instead of maturing and releasing an egg every month, your ovaries get stuck. You might end up with a bunch of small follicles, but not actually ovulate on schedule. That means your cycles get long, super irregular, or go missing altogether.
For fertility, the main problem is simple: No ovulation = no egg = getting pregnant is tough. But it’s more than just your ovaries.
PCOS usually brings along some friends:
-Higher androgens (like testosterone), think chin hair and acne showing up out of nowhere
-Insulin resistance, so your blood sugar is all over the place, you get crazy cravings, and your energy tanks
-Weight changes that seem to make up their own rules
So yeah, it’s your whole hormonal system in a group chat, and sometimes they’re all yelling at each other.
And if you’re thinking, “Great, my body is working against me,” I hear you. But don’t give up, PCOS is treatable. Plenty of people with PCOS get pregnant, either naturally or with a little help.
Can PCOS get pregnant ?

Yep. And I know that sounds too simple, but it’s true.
If you’re Googling “can PCOS get pregnant” at 2 a.m. (been there mentally, you know), you’re usually asking: Do I still have a real shot?
Yes. Many people with PCOS conceive naturally. Others need meds like letrozole. Others may use IUI or IVF. But PCOS does not automatically equal infertility forever.
The real question is usually: are you ovulating regularly, and if not, what’s the most sensible way to get you there?
How to get pregnant naturally with polycystic ovaries?
Ovulation is the goal here. Some people with PCOS still ovulate, just not like clockwork. Others barely ovulate at all unless they get some help. Usually, once you support: Blood sugar balance, Ovulation, Inflammation, your chances of getting pregnant naturally go way up.
But “natural” doesn’t mean you just wait around and cross your fingers. It usually means you combine lifestyle changes, targeted supplements, maybe some meds, and good timing.
And about that story you always hear, “my friend’s cousin just relaxed and got pregnant”, yeah, it doesn’t work like that. You can’t breathe your way into ovulation. Managing stress helps, but it’s not a magic fix.
What’s the best treatment for PCOS fertility?
There’s no one-size-fits-all answer, because PCOS isn’t the same for everyone. But here’s what’s usually on the table:
1. Medicine to trigger ovulation
This is often step one if you’re ready to get serious about trying.
-Letrozole, this is the new favorite in a lot of guidelines. It basically tells your brain to send more follicle-stimulating hormone, which pushes your ovaries to mature and release an egg.
-Clomiphene (Clomid) – the old classic. Some doctors still use it, but letrozole works better for a lot of people with PCOS.
You take these meds for a few days early in your cycle. Your doctor might track ovulation with blood tests or ultrasounds. It sounds complicated, but once you do it, it makes sense.
2. Metformin and blood sugar support
Metformin helps your body use insulin better. For some, it helps regulate cycles and even jumpstart ovulation.
But to be real, metformin alone isn’t a miracle. It works way better if you’re also making small changes – eating regular meals, moving a bit more, that kind of thing.
If you want to dig deeper into insulin and hormones, check out our piece “How To Lower Insulin Levels Naturally.” It breaks things down step by step.
3. Lifestyle changes that actually matter (not just the ones people love to preach)
People love to say “just lose weight,” like it’s a switch you can flip. That advice, by itself, isn’t helpful.
pcos fertility diet?

Balanced meals, packed with protein, healthy fats, and fiber, are key at most mealtimes to keep your blood sugar steady. And when it comes to movement, you know, something you can actually keep up with is what matters – yes, walking totally counts!
Your hormones also do a ton of repair work while you’re asleep, so don’t skimp on sleep. As for stress management, it’s not that stress causes PCOS, but it can definitely make things worse, so finding ways to manage it is super important.
You don’t need to be perfect, though. Just being “better than last month” is absolutely progress.
Fertility options with PCOS
If you’re not getting consistent ovulation, or you’ve tried for a while and nothing’s happening, fertility options with PCOS usually fall into a few lanes.
One lane is ovulation induction meds (like letrozole). Another lane is adding monitoring to see what your follicles are doing. Then you’ve got options like IUI and IVF if you need more help.
And quick opinion – in my experience, the “best” option isn’t the fanciest one. It’s the one that matches your body, your timeline, your budget, and your mental health. Because yes, your nervous system is allowed to be part of the plan.
What if meds aren’t enough?
If letrozole or similar meds don’t get things going, you still have options. One of the most common next steps is ovulation induction with monitoring.
In this approach, your doctor gives you medication to get your ovaries working, then keeps an eye on how things are progressing with ultrasounds and blood work. Sometimes they’ll add a shot to trigger ovulation once a follicle looks ready. You can kind of think of it as a gentle nudge for your ovaries, not a shove.
Another option is IUI – intrauterine insemination. With IUI, the doctor places sperm directly into your uterus around the time you’re ovulating, often in combination with ovulation meds. This can be a really solid next step when sperm quality is decent but not perfect, when trying to time sex is stressing you out, or when you’ve already tried a few medicated cycles with no luck.
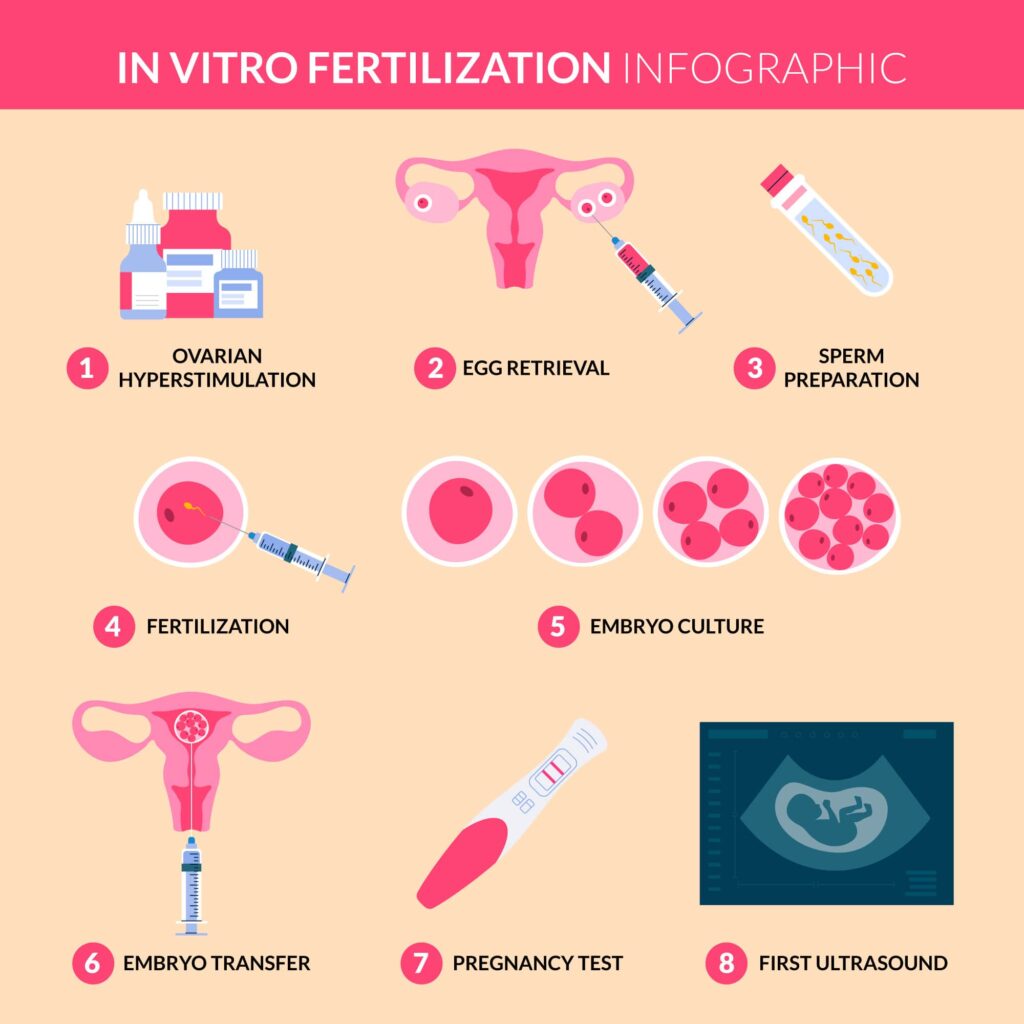
Then there’s IVF, in vitro fertilization, which is the bigger, more intensive option. Here, eggs and sperm meet in a lab, embryos are created, and then one or more embryos are transferred back into your uterus. IVF can work very well for many people with PCOS, though doctors usually monitor closely because PCOS ovaries can react a bit too strongly to stimulation drugs. And needing IVF doesn’t mean you failed or did something wrong – it just means your body needs a bit more support to do what it’s trying to do anyway.
PCOS infertility rate
People ask about the PCOS infertility rate because they want certainty. Like a number that tells them how worried to be.
But PCOS doesn’t give neat little guarantees. Some people with PCOS conceive quickly. Some struggle for a while. A lot depends on whether ovulation is happening, age, sperm quality, and other health factors.
So yes, PCOS is one of the most common causes of ovulation-related infertility. But it’s also one of the most treatable. That part matters, a lot.
So all the effort you’re putting in now? It pays off, way beyond fertility alone. If blood sugar and insulin resistance are clearly part of your picture, you might also want to explore more posts under Supplements for Blood Sugar Control tag on The Hormone Nest – it pulls together content focused on that specific root cause.
PCOS fertility rate with age
Age is the annoying factor nobody wants to talk about, but it matters for everyone, not just PCOS.
PCOS fertility rate with age can be a bit of a mixed bag. Some people with PCOS may have a longer reproductive window because they ovulate less often over time. But that doesn’t mean age doesn’t matter. Egg quality still changes with age, and the risk of miscarriage can go up over time too.
So if you’re trying now and you’re feeling urgency, that’s not “dramatic.” It’s just your brain doing math.
And if you’re younger and you feel pressured to panic, you don’t have to. You just need a plan and some tracking so you’re not guessing in the dark.
References
- Teede HJ, Misso ML, Costello MF, et al. “Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome.” Human Reproduction. 2018.
https://academic.oup.com/humrep/article/33/9/1602/5053706 - Legro RS, Arslanian SA, Ehrmann DA, et al. “Diagnosis and treatment of polycystic ovary syndrome: An Endocrine Society clinical practice guideline.” Journal of Clinical Endocrinology & Metabolism. 2013.
https://academic.oup.com/jcem/article/98/12/4565/2834740 - Palomba S, de Wilde MA, Falbo A, et al. “Pregnancy complications in women with PCOS.” Human Reproduction Update. 2015.
https://academic.oup.com/humupd/article/21/5/575/609125 - Morley LC, Tang T, Yasmin E, et al. “Insulin-sensitising drugs (metformin, rosiglitazone, pioglitazone, D-chiro-inositol) for women with PCOS, oligo amenorrhoea and subfertility.” Cochrane Database of Systematic Reviews.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD003053.pub6
Disclaimer:
This article is for educational purposes only and is not medical advice. It doesn’t replace a consultation with your doctor, fertility specialist, or qualified health practitioner. Always talk to your healthcare provider before starting, stopping, or changing any treatment for PCOS or fertility




